
So Why do Disk Replacement Surgery Anteriorly (from the front)?
Posted on May 14, 2013 by sonjabarrie
19 days and counting till we leave for Barcelona….
You would think that if they are working on your spine they would be working on or operating on your back wouldn’t you?
I’ve been asked a number of times about why my belly will get so big when it’s my back they are working on.
Now, when they operated on my back for the laminectomies they did it from behind because they were taking out the soft pieces of disk that had broken off. The disks usually expand or break off to the sides which means they can be accessed from the back. You also don’t want to go through major surgery just to fish out a small piece of disk (my first piece was almost an inch long, not exactly small). Usually the pieces are about ¼ of an inch but they still hurt none the less.
When we are talking about actually replacing those disks though, that’s another story. The spinal column gets in the way and it’s not like they can cut it and sew it back together!
This animated video shows the process better than all the words I could come up with.
Spinal Kinetics M6-L Artificial Disc Replacement: Surgery Animation
In order to do this they need to cut you from the front and move all those pesky organs out of the way, like your colon and bladder. None of your organs appreciate this in the least and they really let you know about it after the op. Apart from swelling up like a huge pumpkin, your bowels rebel and stop working, your stomach can go on strike and I don’t even want to talk about how the rest of them gang up on you.
Then there is your spinal column, some say as soon as the surgery is done and those awful extruding disks are replaced, their back pain in gone. Others, who have lost disk height, can have problems as the new disks stretch the nerves and muscles back to their original size. This is called distraction pain.
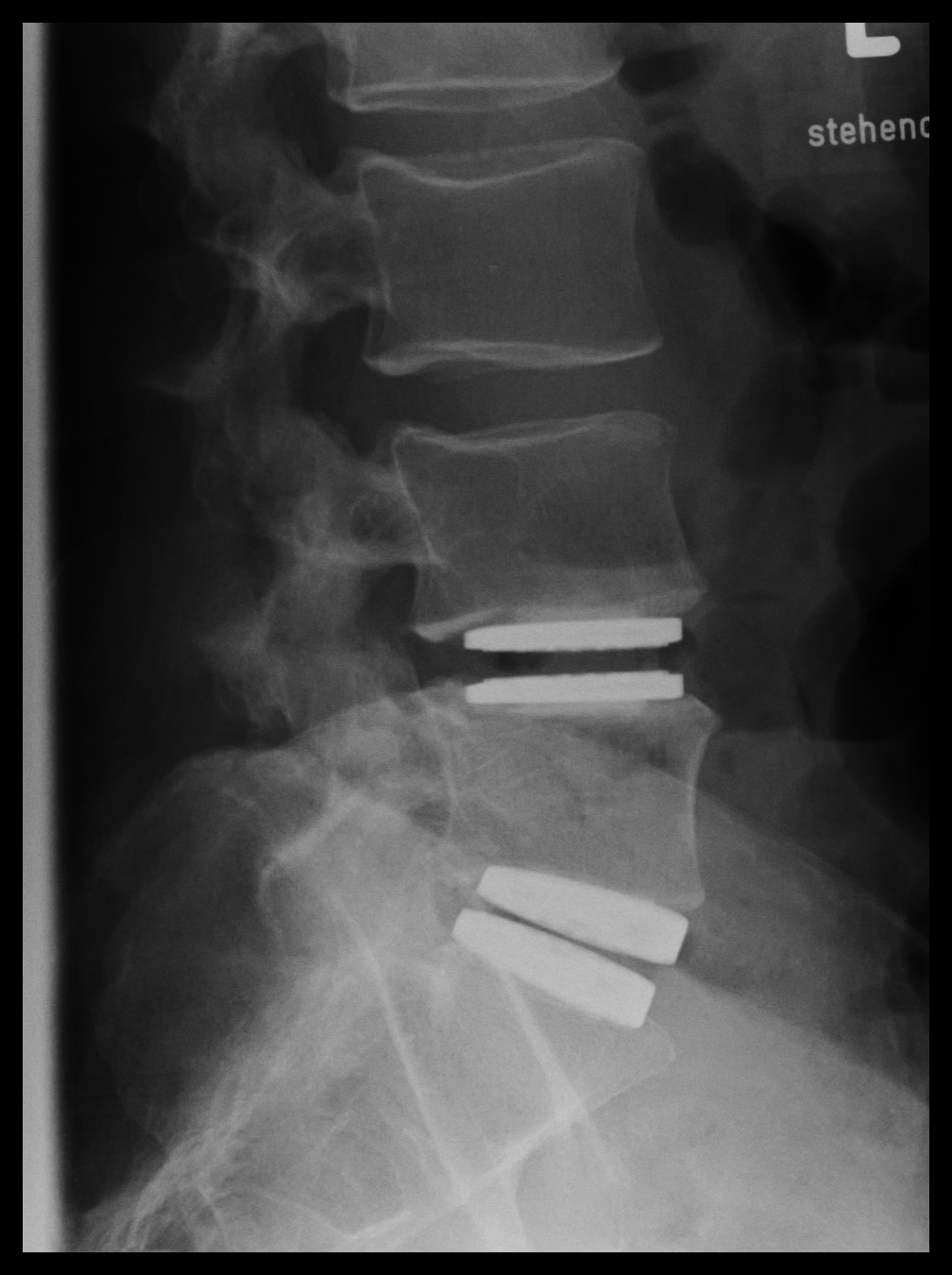
This is what my new back should look like when they are done.
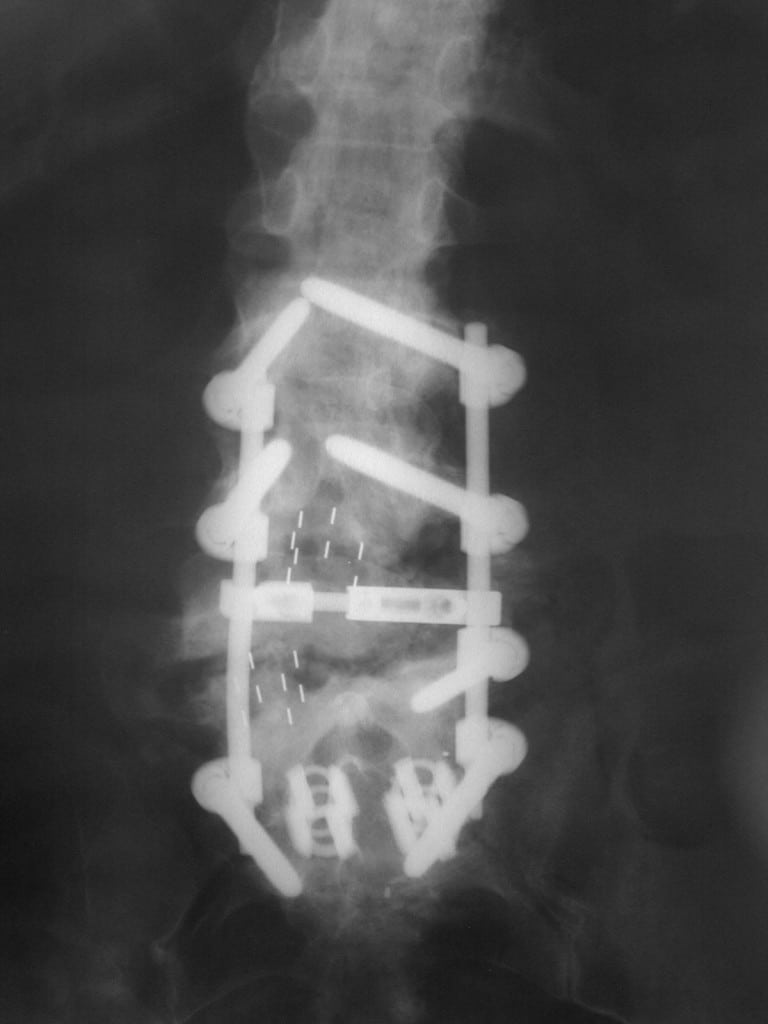
Which is a LOT better than this which is a fusion, every fusion isl different but you get rods, screws, bone implants etc. regardless.
Some really techy stuff
There are 2 approaches when it comes to the actual incision, the transperitoneal or a retroperitoneal approach and each cause your organs to be moved differently. Which is used can be surgeon preference but it can also depend on which disks need to be accessed.
The information on the two approaches are taken from this site, very informative, http://www.acssurgery.com/acssurgery/secured/getChapterByIDHTML.action?bookId=ACS&readerFlag=chapt&chapId=part06_ch33 especially the section on NERVE DYSFUNCTION which guys should read and be aware of.
Retroperitoneal approach
This approach has gained popularity in treating a variety of diseases of the spine. Over the past decade, a broad range of lumbar pathology has been treated with instrumentation requiring an anterior approach. General, vascular, and trauma surgeons are often enlisted to provide exposure of the spine. Anterior fusion and disk replacement procedures have become common, especially with the development of anterior lumbar interbody fusion and total disk arthroplasty. The spinal pathology addressed during the anterior exposures may be divided into diseases that affect the intervertebral disk and diseases that involve the vertebral bodies along with the disk. The most common sites of involvement are the fourth and fifth lumbar vertebrae and the intervertebral disks between L4 and L5 and L5 and the sacrum (S1).
Knowledge of retroperitoneal anatomy is essential to the successful performance of these procedures. The iliac vessels will often need to be mobilized to gain access to the anterior aspect of the lumbar spine. During this mobilization, injury to the vessels may occur. Injuries to the iliac vessels are uncommon; however, when these injuries occur, life-threatening hemorrhage may result. Having a surgeon who can repair these injuries and perform the exposure can potentially reduce the chances of complications and optimize patient outcomes.
TRANSPERITONEAL APPROACH
A standard, transperitoneal open approach to the lumbar spine has been described. In general, the approach may use a lower midline or transverse incision. Instead of dissection proceeding in an extraperitoneal plane, the peritoneum is entered and the bowel is packed. The retroperitoneum is then entered, and the disk spaces are exposed. This dissection has the drawback of bowel manipulation and has been shown to have a markedly elevated incidence of retrograde ejaculation. We have reserved this approach for remedial operations following previous anterior retroperitoneal approaches when the removal of hardware is necessary.
I also found this .pdf which shows the organs though it details an S1 fusion more than a disk replacement.
I have heard on the forums how some suffer from pain in their Psoas muscles after the op, this picture lets you know why! this is what they do to move all your organs.
Anterior Retroperitoneal Spine Exposure




Leave a Reply

{kind=link}